Sympathetic Chain Pathology & Sympathetic Autonomic Hyperactivity: The Importance of Spinal Manipulation in Optimizing Autonomic Nervous System Homeostasis
Sympathetic Chain Pathology & Sympathetic Autonomic Hyperactivity: The Importance of Spinal Manipulation in Optimizing Autonomic Nervous System Homeostasis
https://www.ncbi.nlm.nih.gov/books/NBK539914/
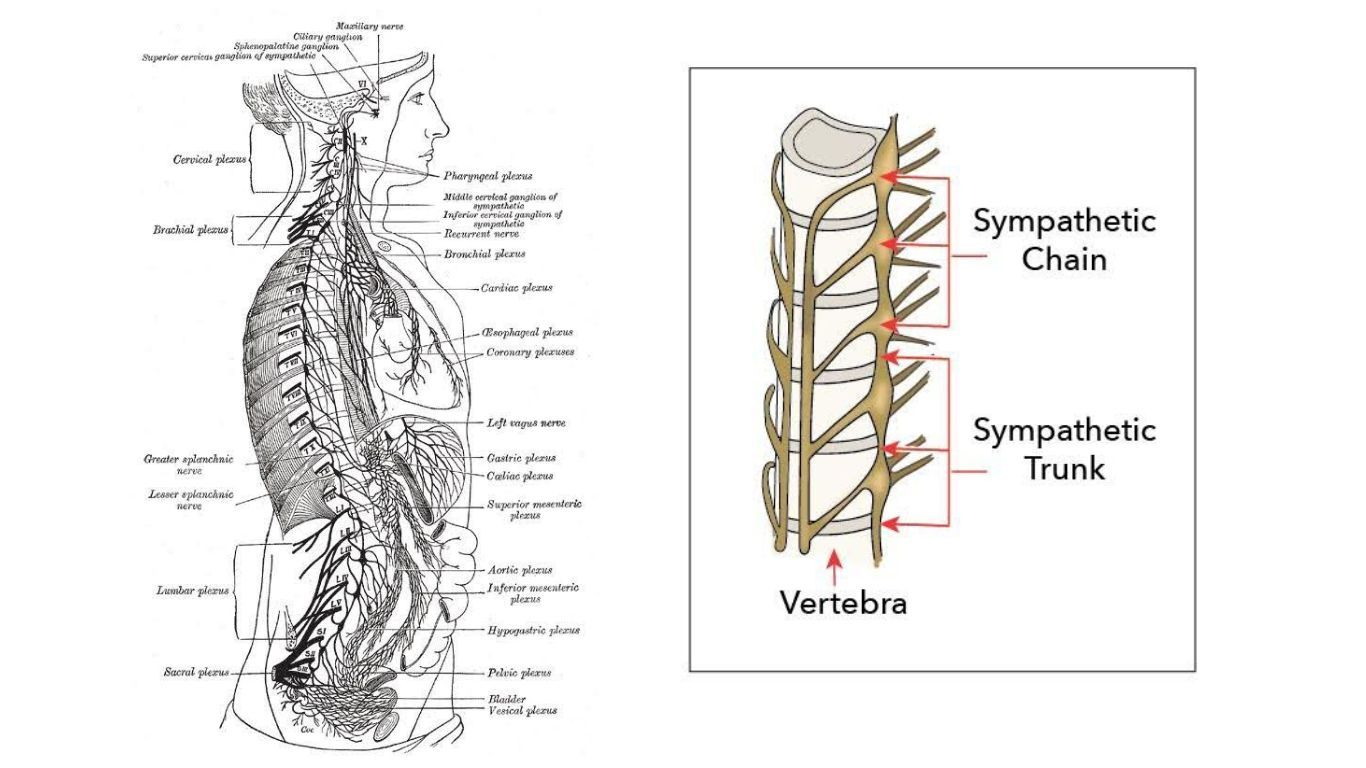
Upper Extremity radicular symptoms without cervical or upper extremity pathology may be frustrating to resolve. This is because the cervical, thoracic, lumbar, sacral, and coccygeal spines are all traversed by 2 long chains of nerves exiting the brain and traveling the entire length of the spine to the coccyx. The sympathetic chain sits on the anterolateral aspect of the vertebral bodies, more or less, and has about 23 ganglia. The stellate (star) ganglion is typically considered the top of the sympathetic-dominant portion of the chain and produces sympathetic efferents to the arms, head, neck, and heart, we think. It sits just on the anterior aspect of the first costotransverse joint at C7/T1. Most anatomy and physiology books denote the sympathetic chain from the stellate ganglion to about L1/L2. Above and below that are the parasympathetic-dominant sections of the chain. The parasympathetic-dominant cranial nerves V, VII, IX, and X above, and the sacral plexus (S2-S4) below. Abnormal tension is imposed upon this chain secondary to muscular and joint pathology anywhere along its length. Any part of the brain and body may present with pathology secondary to tension anywhere along the entire chain. Headaches, anxiety, heart palpitations, dizziness, brain fog, fatigue, fibromyalgia, hiccups, incontinence, and more nasty stuff may result.
Sympathetic autonomic hyperactivity leads to dysfunction of the hypothalamic-pituitary-adrenal (HPA) axis, the gut-brain axis (enteric nervous system and brain connected primarily by the vagus nerve and sympathetic chain), and the trigeminocervical complex, all key components of the autonomic nervous system. Without homeostasis of these pieces of the autonomic system, our hormones, immune system, neuromodulators, peptides, DNA transcription, etc., all become dysregulated. This is bad.
The fastest, easiest way to reduce tension on the sympathetic chain is to first dry needle the appropriate structures to push the autonomic nervous system into parasympathetic dominance to reduce muscle tension and spinal compression, then manipulate the spine back to neutral. With my first needles, I target the parasympathetics: auricular branch of the vagus nerve, base of the occiput, cranial suture lines, sacral plexus, pelvic floor; then I needle the multifidus, iliopsoas, latissimus, paraspinals, QL’s, and any other tight stuff I find. Then I treat all the hypomobile joints I find.
Many physical therapists are hesitant to perform spinal manipulation, especially regarding the cervical spine. If manipulation is performed properly, the structural stresses placed on the cervical neurovasculature are far less than we place on the same structures ourselves a hundred times a day, just by living life. A completely misunderstood aspect of cervical manipulation is what is actually taking place on an arthrokinematic level. When I perform cervical manipulations, I am never taking any individual joint past about 50% of its total range.
The C3-C7 cervical joint facets sit at about a 45-degree angle. If you are sitting or standing, stick your arms straight out in front of you, then elevate them up 45 degrees – that is about the plane the cervical facets move in. They move up and forward and down and back in that spacial plane. Put your arms straight back out in front of you, and that is the plane the subcranial spine (C0-C2) moves in. The horizontal plane, more or less. When manipulating any joint, they should primarily only be moved along the plane they live in, or perpendicular to that plane, into distraction. In the cervical spine, this is especially important to avoid excessive neurovasculature stress.
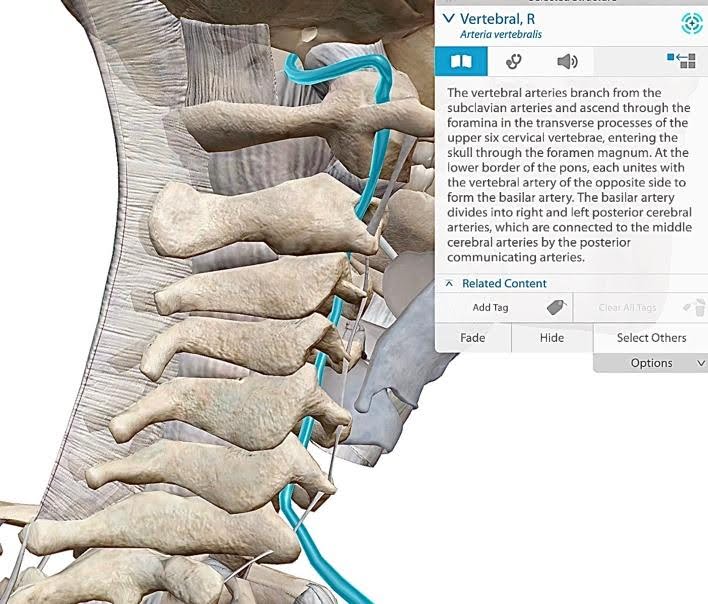
When manipulating the middle and lower cervical spines, C3-C7, the neck should be in side-bending and rotation to the opposite side. This is to place the facets in approximate neutral when the manipulation is performed. Normal C3-C7 arthrokinematics are side bending and rotation to the same side. The thoracic and lumbar spine typically side-bend and rotate to opposite sides. If you bend your head all the way to the side and you can keep your eyeballs straight ahead, which you should be able to do, this is only possible because as the right C3-C7 facets are sliding down and back and rotating to the right, C2 in counterrotating to the left. The more downslide or upslide the cervical facets are in, the more kinked and stressed the vertebral artery is running through the transverse foramina. Stress on the vertebral artery tends to be the primary objective studied in the manipulation literature for safety concerns.


Many instructors teach to manipulate the cervical spine by placing the impulse through the articular pillar (in between spinous and transverse processes) down toward the contralateral armpit. However, this shears the facet joints down and sideways, a direction the facets never move on their own. This direction of facet movement only happens during a car accident, or when getting run over by an NFL linebacker. Basically the same thing. The natural direction facets travel in during activities of daily living is up and forwards or down and back. As the right facets move up and forward during left cervical rotation or side-bending, the lefts facets slide down and back. Right facet upslide and left facet downslide occur concomitantly, with slight deviation towards center. Subsequently, this is the direction in which the joints should be manipulated. However, the cervical facets must be moved in side-bending and rotation to the opposite side, prior to manipulation.
The neurovasculature in the neck we don’t want to push on are situated from the transverse processes forward. This makes it unreasonable to push or pull from the front side of the transverse processes. Therefore, our remaining option is to find the transverse processes and facets that are hypomobile and either pull or push them up and forward. In performing cervical manipulations in this manner, we can reduce cervical joints to neutral by manipulating them from neutral, and place significantly less stress upon the cervical neurovasculature than we do during end-range passive range of motion throughout the day.
The sensation perceived through the hands of the practitioner prior to cervical manipulation should be when maximal facet opposition is reached, or joint neutral. Although the head and neck are not in neutral, the joints are. Since the capsules normally move in side-bending and rotation to the same side during activities of daily living, by moving the joints in side bending and rotation to the opposite side along the natural plane of the facets, one facet moving up and forward and the contralateral facet down and back, we twist and tension hypomobile facet capsules more quickly than non-restricted ones. In this manner, with proper instruction and practice, adequate tension of the joint capsule is achieved when the facets and transverse foramina are more or less in neutral. This allows a practitioner to manipulate the cervical spine and achieve joint cavitation without placing any joints much past mid-range of motion. Remember, simply turning your head all the way to one side far exceeds the neurovascular stress induced during this style of manipulation.
Without optimal neutrality of the spinal column, the sympathetic chain will always be stressed. Because of the chain’s anatomic location, it is simply impossible to deviate a spinal segment without stressing it. If the sympathetic chain is stressed to any degree, pathologic afferent autonomic signals are continuously sent to the brain. Enough negative sympathetic afferent signals from one location, or combined from numerous locations, leads to chronic sympathetic autonomic nervous system hyperactivity. This is detrimental to all aspects of physical and mental health.
Sign up for, or host a manipulation or dry needling course: https://intricateartseminars.com/
Thanks for reading. Let me know if anyone has any questions about anything.
Jason
References
- Piper SL, Howarth SJ, Triano J, Herzog W. Quantifying strain in the vertebral artery with simultaneous motion analysis of the head and neck: a preliminary investigation. Clin Biomech. 2014;29(10):1099–107.
- Dunning, J.R., Cleland, J.A., Waldrop, M.A., Arnot, C., Young, I., Turner, M. and Sigurdsson, G., 2012. Upper cervical and upper thoracic thrust manipulation versus nonthrust mobilization in patients with mechanical neck pain: a multicenter randomized clinical trial. journal of orthopaedic & sports physical therapy, 42(1), pp.5-18.
- Tsegay, G.S., Gebregergs, G.B., Weleslassie, G.G. and Hailemariam, T.T., 2023. Effectiveness of Thoracic Spine Manipulation on the Management of Neck Pain: A Systematic Review and Meta-Analysis of Randomized Control Trials. Journal of Pain Research, pp.597-609.
- Young, I., Dunning, J., Butts, R., Bliton, P., Zacharko, N., Garcia, J., Mourad, F., Charlebois, C., Gorby, P. and Fernández-de-Las-Peñas, C., 2023. Spinal manipulation and electrical dry needling as an adjunct to conventional physical therapy in patients with lumbar spinal stenosis: a multi-center randomized clinical trial. The Spine Journal.
- Dunning, J., Butts, R., Zacharko, N., Fandry, K., Young, I., Wheeler, K., Day, J. and Fernández-de-Las-Peñas, C., 2021. Spinal manipulation and perineural electrical dry needling in patients with cervicogenic headache: a multicenter randomized clinical trial. The Spine Journal, 21(2), pp.284-295.
DISCLAIMER: The content on the blog for Intricate Art Spine & Body Solutions, LLC is for educational and informational purposes only, and is not intended as medical advice. The information contained in this blog should not be used to diagnose, treat or prevent any disease or health illness. Any reliance you place on such information is therefore strictly at your own risk. Please consult with your physician or other qualified healthcare professional before acting on any information presented here.
Stay Engaged With Intricate Art
Get the latest news, updates and offers from Intricate Art delivered to your inbox.