Dry Needling for Erectile Dysfunction, Incontinence, Vagus Nerve Stimulation, & Men’s Pelvic Health
Dry Needling for Erectile Dysfunction, Incontinence, Vagus Nerve Stimulation, & Men’s Pelvic Health
The Awesome Efficacy of Thoughtful Dry Needling & Joint Manipulation in Resolving Pelvic Impairment via Autonomic Nervous System homeostasis
Before we begin, let’s clear something up. I know a lot of you are thinking, did he just mention needles and something about the pelvic floor in the same sentence? You want me to do what now? You may be wondering, is he delusional? Confused about where the pelvic floor muscles are located? Someone gave this dude a degree? These are legitimate questions to pose when someone is encouraging you to stick sharp pieces of metal near your Johnson, I hear ya. I am sensitive to needles all over my body, I’ve always had a strong reaction to them. However, the first time I was needled in my pelvic floor, I was shocked. Not literally. It is basically painless. It is, by far, the most comfortable area of my entire body to be needled. I get needled there a lot in our pelvic floor classes and I barely feel them. It also makes you very relaxed following treatment. I realize this sounds completely counterintuitive, it is, but pelvic floor needling is astonishingly comfortable and wonderfully effective for a multitude of impairments.
Introduction
All 9 of the true pelvic floor muscles are innervated by the sacral plexus, S2-S4, to some degree or other. This is one of the parasympathetic dominant potions of the spinal cord, which we can access by stimulating the nerve roots through the sacral periosteum and the muscles innervated by the sacral plexus, the pelvic floor muscles. I like to use 1 Hz microcurrent. Low frequency stim, 1-5 Hz, has consistently been shown to induce elevated levels of endogenous opioids, beta endorphins, to be released from the hypothalamic-pituitary-adrenal (HPA) axis, one of the main axes of the autonomic nervous system. Beta endorphins are potent analgesics that work in depressing pain and the sympathetic autonomic nervous system (SANS), this is key. Almost all physical therapy (PT) patients present with SANS hyperactivity. The mind and body’s natural response to any type of mental or physical pain, stress, trauma, etc., is to elevate sympathetics. Most humans are living with chronic SANS hyperactivity, which is detrimental to all aspects of health, mental and physical.
This being the case, it behooves us to address the opposite part of the autonomic nervous system (ANS), the parasympathetic autonomic nervous system (PANS), which when stimulated, reciprocally inhibits the SANS, leading to autonomic homeostasis, the key to health. One of the best areas to needle to achieve parasympathetic stimulation is the pelvic floor. This is why treating the pelvic floor is so important for all aspects of general wellbeing, not just pelvic floor problems. If you have a pathologic pelvic floor, which I promise you most people do, whether you are conscious of it or not, your ANS is going to be constantly bombarded by negative afferent signals coming from the short, tight, hypoxic, grumpy muscles. This leads to chronic sympathetic stimulation, parasympathetic depression, and ANS dysfunction.
Thoughtful dry needling combined with joint manipulation are the two most powerful tools in Physical Therapy Land to induce ANS homeostasis. And they are safe, cheap, and easy. I don’t know of any medicine that works on basically 100% of people, like the combination of these two treatments. It really does, especially if you understand how to target the ANS in the correct manner and treat the body as a whole complex, interconnected, system. All humans benefit from a more homeostatic ANS. To accomplish this, the PANS needs to become a specific target. More on that in a bit. Along with targeting the parasympathetics, the sympathetic stressors throughout the body, not just in the local area of complaint, must be removed. For example, stress on the sympathetic chain is an underappreciated, systemically destructive problem that causes chronic sympathetic autonomic hyperactivity and is easily addressed with electrical dry needling and joint manipulation.
To treat and remove these sympathetic stressors, I like to needle pathologic tissue throughout the body, then reduce deviated joints throughout the spine and extremities to neutral. I know this may seem overly simple to many of you, and I agree. This is a very simple, nonpharmacologic treatment, that works awesome and has wide ranging health benefits for most of humanity. There is no person that has perfectly healthy tissues throughout their body. The more abnormal tissue you have, like tight muscles, trigger points (knots), joint stiffness, etc., the more chronic sympathetic stimulation your brain is receiving. Chronic sympathetic hyperactivity may present in numerous ways, sorta like a chameleon, you know? Changes colors based on its environment. Well, people’s nervous systems change their color, or flavor, if you will, based on a lot of environmental and neurophysiologic factors, and everyone is different. Chronic sympathetic hyperactivity is often expressed as a combination of mental and physical impairments, which entangle into a negative feedback loop that must be broken in order to return the ANS toward homeostasis and allow the body and mind to heal themselves and function at maximum performance.
This is a key point to understand. The way most medicine works is through addition. We give people medicine to fix problems. This is how MD’s are trained because it’s how pharma companies make their money, with which they bribe, I mean fund, the government, and that is how research and universities are funded. It’s all very convoluted. I’m not saying pills are bad, all the time, but things have gotten out of control. What is not profitable, in a monetary sense, is simply subtracting, removing, physical stressors to the SANS, while at the same time, stimulating the PANS with various methods we will discuss further along in this discussion.
I bring this up because many people disregard seemingly simple things like sticking a tiny needle into tissue, without any medicine, and moving joints around so they are where they should be. This is a mistake. Removing a significant amount of SANS stress coming from joints and tissues, especially in conjunction with targeted PANS stimulation, has a profound regulatory effect on the ANS, nudging it toward homeostasis. ANS homeostasis helps the body maximize and utilize its mind boggling, innate ability to heal. This is the cool thing about these treatments. Instead of a pill to mask the symptoms of a problem, we are removing stress from the body, which removes stress from the mind, which allows the brain to heal and regulate the body to its full potential. The power of this cannot be understated.
Without significant underlying pathology, like spinal cord injury, uncontrolled diabetes, structural damage, morbid obesity, or other bad stuff, no man should suffer pelvic health issues. Even in those instances, improvement is possible. Unfortunately, it is estimated that 40% of all 40-year-old men have some form of erectile dysfunction (ED). That number increases 10% per decade. That means 60% of guys in their 60’s are gonna have some form of dysfunction. Mind you, this only accounts for erectile dysfunction. Think about the numbers when all pelvic health impairments are added in. Ummmm….. I don’t know about you guys, but I plan on having a fully functional weewee throughout life, without medication. You should too. Don’t laugh, well do laugh at “functional weewee”, that is funny, but seriously, I know a lot of guys reading this are likely thinking there is no hope. I get it, many of you have tried treatment options with little to no success. Don’t despair! Again, unless you have some type of significant underlying pathology, nobody should be suffering from ED or any other pelvic health impairment.
The tricky part is finding a medical practitioner who treats male pelvic health impairments, who treats with thoughtful dry needling and joint manipulation, and who understands pelvic health and its relation to sympathetic autonomic nervous system hyperactivity. Unfortunately, this is not easy. Most physical therapists are female, there is a scarcity of female pelvic health practitioners, and the few who are specialized typically do not treat men. A primary reason for the lack of male pelvic health treatment, at least in physical therapy, is the American Physical Therapy Association (APTA) has 10 specialty board certifications, one of them being Women’s Health. Guess what’s not a specialty? Yup, Men’s Health is nowhere to be found. Why? Based on the numbers, there are somewhere around 60 to 80 million men in the United States suffering from pelvic health impairments. The majority suffering needlessly. Makes total sense to completely disregard a large swath of medical impairments about a quarter of the population suffers from. Not to mention the secondary mental health issues commonly associated with pelvic health impairment. Sound reasoning…
Remember, the human body’s typical response to mental or physical stress, strain, trauma, etc., is sympathetic autonomic nervous system (SANS) elevation. Chronic SANS hyperactivity is detrimental to every aspect of health, including pelvic health. Overall, the most sure-fire, simple way to maintain ANS homeostasis and overall health throughout life is not eating too much, eating well, and staying in shape. The problem with that is, most people eat way too much, what they do eat is garbage, and never have or will exercise. What a conundrum. Therefore, we must find alternate, preferably nonpharmacologic treatments to achieve ANS homeostasis. The best treatment I know of is thoughtful dry needling combined with joint manipulation. The results are stunning, even for me, and I see this stuff all the time.
Vagus Nerve Stimulation

Auricular Vagus nerve stimulation should be a widespread physical therapy treatment for most medical impairments. It is a powerful ANS regulator. Unfortunately, it is not. Acupuncture boards, and some PT boards, which is sad, erroneously believe or state needling the ear is acupuncture. Keep in mind, PT’s are ‘allowed’ to stimulate the vagus nerve, in all states that I’m aware of, without the use of needles; so it is simply the addition of the needle which is in question. No one profession owns a body part or a tool and we should work in unison in order to benefit all.
Acupuncture is based on a theory including some 300-plus specific acupuncture points, with 12 or so meridians, energy lines. This energy is the “chi” you hear about acupuncturists balancing. Neither the points nor the meridians have ever been proven to exist, which doesn’t mean they are not there, by the way. That line of thinking will lead you right into a sewage filled cesspool of stifled mental function. Acupuncture has been around for thousands of years. Things that don’t work do not persist through millenia. Acupuncturists somehow use a combination of the points along the various meridians to balance the energy. Now, energy lines certainly do exist in our body, if we didn’t have energy flowing throughout our body, we’d be dead. When acupuncturists say they are balancing meridians, what they are attempting to accomplish, I believe, is ANS homeostasis. This is the same thing I aim to achieve with my patients, using the same tool, a tiny needle. The primary difference is, well, everything else. I am using my knowledge of neurophysiologic processes along with human anatomy to directly affect change in order to achieve a specific neurophysiologic goal, ANS homeostasis and improved health. For the vast majority of recorded human history, acupuncture has been around. What has not been around, until the last hundred years or so, is our current idea of neurophysiology. Like, it didn’t exist. Again, to equivocate dry needling to acupuncture, anywhere in the body, is to imply a substantial lack of understanding regarding either treatment approach. This roadblock/restriction on one body part needs to be addressed, as PT’s in certain states are being actively prohibited by their own boards from helping their patients as much as possible. According to the APTA, dry needling is used to treat neuromusculoskeletal impairments. I challenge anyone to explain how targeting the vagus nerve and the PANS with needles does not fall under that definition.
That was not a rant, by the way. I am just clarifying things that obviously need clarification… Anyway… What is a common link for basically all PT patients? Sympathetic autonomic hyperactivity. Regardless of the initial cause of the problem, sympathetic hyperactivity and its various detrimental downstream effects are often the driving factor limiting our awesome, innate ability to heal. The worse physical and mental condition we are in and the older we get, the harder it is for our ANS to self-regulate following disruption. Putting it very simply, this is why we heal worse and slower as we age. So, if sympathetic activity reciprocally inhibits parasympathetic activity and vice versa, what is the best way to reduce sympathetic activity? Target the parasympathetic autonomic nervous system. What is the most direct means of achieving this? Electrical dry needling targeting the vagus nerve, along with other specific mental and physical factors stimulating sympathetic activity.
The auricular branch of the vagus nerve, cranial nerve X, innervates multiple areas of the ear. This is the most direct, powerful PANS-specific treatment we can perform. The Vagus nerve is sometimes referred to as the “wandering nerve” because of its meandering path leading from the brainstem to the heart, organs, intestines, aorta, and more. It innervates a lot more unique structures than any other nerve I’m aware of. It is the primary nerve of the PANS and about 80% of the nerve fibers are afferent, indicating its main job is to tell the brain what is going on in our organs and other subconscious bodily functions, so our brain can monitor and regulate what is going on. The vagus nerve gives our brain interoceptive awareness, or awareness of what is going on inside our body.
3 Common Vagus Nerve Ear Distributions to Target & Regulate the Autonomic Nervous System Toward Homeostasis:
- Concha
- Cymba Concha
- Inner Tragus

Targeting the parasympathetic autonomic nervous system with needles has a homeostatic effect on the ANS via sympathetic depression and other neurophysiologic mechanisms. We know so little about the mechanisms of action that lead to this, but we do know the overall result of vagus nerve and parasympathetic-specific needling. SANS depression and ANS homeostasis, at least compared to baseline. There is good research looking at surgical vagus nerve stimulation with a metal cuff placed around the nerve itself, and good acupuncture research looking at vagus nerve stimulation via its auricular distribution in the ear. A recent meta-analysis found high efficacy in depressing sympathetic hyperactivity and bringing the ANS towards homeostasis in both auricular stimulation and surgical implantation. Obviously better to avoid surgery.
The amount of research on vagus nerve stimulation has significantly increased over the last few years, which is awesome. Hopefully this becomes a widespread treatment for a multitude of mental and physical impairments. It certainly should be. Auricular vagus nerve electrical dry needling consistently produces incredibly powerful results in my patients. An awesome thing about this is it works for a wide range of medical impairments. All conditions do better with a more homeostatic ANS, and stimulating the vagus nerve is the most powerful place we can access with needles to directly induce ANS homeostasis. It helps regulate the primary axes of the ANS, the hypothalamic-pituitary-adrenal (HPA) axis and the gut-brain axis (enteric nervous system + brain). Remember, the gut plays a large role in regulating mood, serotonin, dopamine, immunity, and we are learning more and more about how important it is all the time.
To maximize treatment efficacy and ANS homeostasis, it is important to include low frequency (1-5 Hz) microcurrent. It really helps. Remember, don’t use regular stim with needles, people will not like you, it hurts, too many amps. 1-5 Hz has consistently shown across electrical research to be the best frequency to stimulate endogenous opioid (beta endorphin) release from the hypothalamic-pituitary-adrenal (HPA) axis. Up to 4 times the amount of beta endorphin becomes accessible when using low frequency stim with your needles. Beta endorphin reduces pain, which alone reduces sympathetic activity. It also has other mechanisms of action that we are trying to understand. I like to use 1 Hz microcurrent, closest to normal heart beat, and connect the parasympathetic dominant areas of the body to each other, in various ways. The other 2 parasympathetic-dominant locations to access with electrical dry needling are the sacral plexus, S2-S4, and the suboccipital periosteum / C2 spinous process. Placing current through periosteal tissue and needling bilaterally are things I do as often as possible, it appears to induce a more powerful homeostatic, healing effect.
I place 3 needles in each ear, or in one ear if that is all I can access, as the first needles of my treatments. I then place needles in the other 2 areas I mentioned above, depending on patient position. Then I treat whatever else I am going to, hook up the microcurrent, and leave the patient for 20-30 minutes. Leaving the needles in place for over 20 minutes is ideal.
Vagus nerve stimulation is FDA approved for anxiety, epilepsy, and depression. You know what two common mental issues are recognized by the FDA to consistently cause sexual performance problems, including erectile dysfunction? Anxiety and depression. Therefore, shouldn’t the FDA, by extension, approve vagus nerve stimulation for erectile dysfunction? Vagus nerve stimulation is being studied for chronic pain, eating disorders, drug addiction, ADHD, and more. This is a poorly tapped resource that, theoretically, should help, to some degree or other, with the vast majority of medical impairments. I base this on the fact that most people live with sympathetic hyperactivity and all medical impairments, mental and physical, to my knowledge, improve with a more homeostatic ANS.
How is this simple, safe, cheap treatment not a standard of care? Well, precisely because it is cheap, easy, safe, and potently effective for a large swath of medical maladies… Makes perfect sense, if the only thing you care about is your bottom line…. By implementing this practice into your existing treatment methods, you will see awesome, wide ranging mental and physical improvement of impairment, including men’s pelvic health impairments.
Related: Check out another of my articles on vagus nerve stimulation & autonomic nervous system homeostasis:
Erectile Dysfunction
Vagus nerve stimulation, along with other needling treatment, has excellent effects on reducing erectile dysfunction, again, through ANS regulation. The main problems with erectile dysfunction are blood flow and muscle tonicity. Not enough blood flow and hypoxic, tight, short, dysfunctional muscles. These 2 things almost always accompany each other and are both classic signs of sympathetic autonomic hyperactivity throughout the body. Remember, sympathetic hyperactivity constricts the endothelial smooth muscle lining of arteries, elevates blood pressure and leads to muscular trigger points, shortening, hypoxia, and widespread neuromusculoskeletal dysfunction. To counter sympathetic hyperactivity, the aggravating sympathetic stimulation must be removed locally and throughout the body (pain, short muscles, displaced joints, knots in muscles, etc.), while at the same time targeting and elevating the parasympathetics.
The two primary muscles needed to achieve erection are the ischiocavernosus and the bulbospongiosus.

These muscles, along with other muscles and structures, need to be supple and able to fill with blood. With enough blood flow, the venous valves in the penis passively close, keeping it filled with blood, erect. If these muscles are short and hypoxic, they do not sufficiently fill with blood. Short, hypoxic muscles also cannot contract properly, further hindering erection. Chronic sympathetic hyperactivity leads to dysfunctional tissue body wide, along with a bazillion other negative consequences like hormone imbalance, immune dysfunction, decreased neuroplasticity, stifled mental and physical well-being, hyperalgesia, allodynia, and more.
A few of the most objective facts we have discovered about thoughtful needling are that it normalizes tissue length and significantly increases blood flow, via autonomic nervous system homeostasis. These just so happen to be the major limiting factors in achieving and maintaining an erection. We know a bit about what happens to incite these changes. Sympathetic depression and parasympathetic elevation both vasodilate arteries through various mechanisms. One of the more well-known parasympathetic mechanisms for this, aside from overall inhibition of sympathetics, is calcitonin-gene-related-peptide (CGRP) release and regulation, a potent vasodilator. Needling the pelvic floor and other structures restores normal tissue length and physiology, improves nerve conduction velocity, muscle strength, blood flow, power, firing patterns, and overall function.
Again, we are pretty good at seeing and measuring cause and effect in medicine. What we are not good at is understanding, or often even seeing in the first place, all the stuff that happens in between the cause and effect. For example, we know tissue heals with the help of scar tissue formation, collagen deposition. However, we are currently discovering brand new forms of collagen in the human body, showing a lack of basic understanding about the mechanisms of tissue healing. We do not even know exactly how muscles contract. On top of that, much of what we currently believe to be true will undoubtedly be proven false in the future. All of scientific history is riddled with examples of this. I mean, seriously, we were performing barbaric lobotomies not that long ago. It’s fascinating to ponder.
In our case, concerning male pelvic health, the cause of the changes is dry needling combined with joint manipulation. The effect, total awesomeness. I see decades of impairment eliminated in a handful of treatments a lot of the time. However, specifically how the awesomeness is achieved, how all the different neurophysiologic mechanisms intricately interact with each other to achieve the end result, is poorly understood. It would be clinically beneficial and super interesting to understand precisely how and why all these positive healing responses occur, but we are a long way from that. Almost certainly, the overall effect is due to increased autonomic nervous system homeostasis amplifying our body’s magical, innate ability to heal. In the meantime, as we continue to learn and discover, understanding that things work, even though we don’t know most of the why things work, will have to suffice. And these treatments, with the proper knowledge, work amazingly well.
Keep in mind, no systemic or bodily changes are possible, aside from the physical puncturing or stressing of tissue, without the nervous systems modulating said change. These changes are orchestrated in various parts of the brain. The HPA axis plays a central role in maintaining our overall well being via autonomic nervous system homeostasis. The HPA axis is one of the two major axes of the ANS, the other being the gut-brain axis (enteric nervous system + brain). Every human condition thrives with a more homeostatic autonomic nervous system, including erectile dysfunction, and the combination of these treatments achieves that better than any other treatment I know of.
Related: Check out another article on male pelvic health, ED, & ANS homeostasis:
Incontinence
Incontinence and erectile dysfunction often accompany each other, although not always, as both typically result secondary to the same underlying dysfunction, chronic sympathetic hyperactivity and autonomic nervous system dysregulation. Do you see a pattern here? Similar to erectile dysfunction, incontinence is typically due to overactive sympathetic activity in various brain and body areas, which leads to abnormal afferent and efferent signals to structures necessary in maintaining continence, resulting in incontinence.
There are numerous areas in the brain we have affiliated with incontinence. For urinary incontinence, one of the primary control centers is thought to lie in the pons, the pontine micturition center (PMC). fMRI studies have demonstrated consistent spontaneous sympathetic electrical firing in the PMC in people with urinary incontinence. Studies have also demonstrated the potent homeostatic effects proper needling has on the PMC and other brain regions by reducing sympathetic hyperactivity and nudging the brain and body toward homeostasis.
Like erectile dysfunction, incontinence is a result of the same negative feedback loop. In both instances, there are numerous ways the impairment may begin. It may begin physically, mentally, or most commonly, a combination of both. Mental problems cause physical manifestations and vice versa. This is why it is vital to treat mental and physical well being together, in a coordinated, insightful manner. Anyway, regardless of the initial cause of the problem resulting in ED or incontinence or whatever, at a certain point, the autonomic nervous system reaches sufficient dysfunction to the point of no return, without specific intervention. This point of no return is easier to reach the more unhealthy we are and the older we get. The threshold of stuff our brain can adequately deal with goes down. Once this threshold is reached, the body loses its ability to heal itself, without a little help. The sympathetics continue in perpetual hyperactivity, muscles get tighter, shorter and hypoxic, blood flow is diminished, functional muscle contraction and relaxation is inhibited, everything hurts, all of which further aggravate the SANS, and the cycle continues, leading to leaking whiz and deflated dingalings (my personal terms). Two things best avoided.
To accomplish this, the pelvic structures themselves, including applicable associated structures throughout the body, which change based on the patient, along with the parasympathetic-dominant portions of the ANS, must be treated with the express intent of using that connection to help effectively eliminate incontinence and erectile dysfunction. The best treatment, often the only treatment that succeeds, is the thoughtful combination of dry needling and joint manipulation. Enough of the sympathetic stressors throughout the body need to be eliminated to reduce the overall aggravation to a point where the body can once again self regulate. Needling and joint manipulation is the best way to achieve this.
Pelvic Pain
Ever felt like a grumpy gorilla is squeezing your nuts? How about the feeling that someone is taking an ice pick and trying to skewer your rectum? Peeny pain? A painful purple peeny plus a nut-grabbing gorilla? I have experienced all these, and let me tell you, that last one, whoa Nelly! Just contemplating going through any of that again makes me wanna projectile vomit, maybe cry a little… Don’t worry though! This is all horrible, unpleasant stuff, but luckily for us, it’s easily fixable, barring significant underlying pathology.
Pain, mental and physical, although commonplace, is at best, poorly understood. Think about how many people suffer from chronic pain. Much of the time, chronic pain does not have any obvious, singular cause. Pain can be created in the brain with complete absence of physical trauma. So, when people tell you it is all in your head, whether or not they believe you or actually understand what they are saying, they are correct. Physical damage does not directly cause pain. The nervous systems’ response to physical damage is what elicits a pain response and what we experience as pain. A hallmark sign of chronic sympathetic autonomic hyperactivity is widespread pain and inflammation, with or without obvious injury. Tumor necrosis factor alpha (TNF-a), interleukins (IL-1 and IL-6), cortisol, and other proinflammatory substances are released in excessive concentrations secondary to chronic sympathetic hyperactivity. Autoimmune diseases, obesity, diabetes and almost all health impairments consistently present with elevated proinflammatory markers and depressed anti-inflammatory mechanisms, such as the nRF2 pathway. Systemic inflammation is detrimental to healing, neurophysiologic function, and overall well being. Needling and manipulation have been demonstrated to regulate these factors.
Beta endorphin release, a potent endogenous opioid primarily released from the hypothalamic-pituitary-adrenal (HPA) axis, plays an important role in decreasing pain, which dampens sympathetics. Beta endorphin is released in 4X the typical concentration following electrical dry needling with 1-5 Hz microcurrent. It also has other mechanistic homeostatic roles, aside from pain reduction, that are important, but poorly understood. Some white blood cells, for example, release beta endorphin, but we do not understand why.
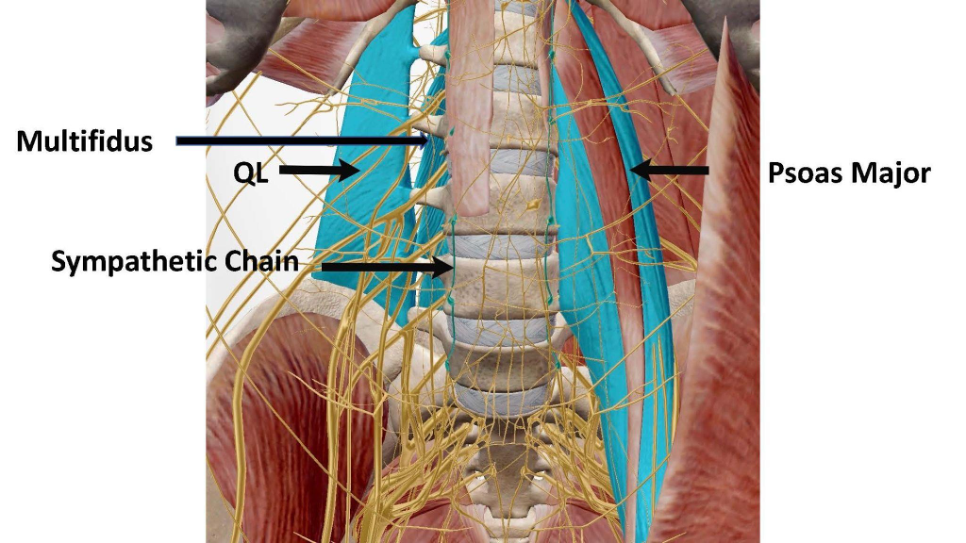
One goal when treating pelvic pain should be to decrease tension on the sympathetic chain by needling the multifidus, psoas, QL, and scalenes, followed by correcting spinal and other joint deviations, placing the muscles and joints in normal anatomic position. The sympathetic chain, the sympathetic-dominant portion of our ANS, sits on the anterolateral aspect of the vertebral bodies in the thoracic and lumbar spine. The multifidus and the psoas major are the two closest muscles to the sympathetic chain in the thoracolumbar spine we can safely access. The psoas major is the deepest muscle on the anterior spine and the multifidus is the deepest muscle on the posterior spine. The sympathetic chain sits directly in front of the psoas major, with tendrils passing through it. The psoas major and multifidus kinda make a sandwich out of the thoracolumbar transverse processes, and the QL attaches to the lateral edge of the transverse processes.
The close proximity of these muscles to each other allows for some type of neurochemical crosstalk between them, meaning when one malfunctions, it is likely the others will as well. Not to mention, pathology of any one of these muscles, since they all attach directly to the spine, will deviate the spine. A deviated spine, in turn, places abnormal tension on the other muscles and the sympathetic chain, making them all pathologic. In pathologic states, the multifidus, QL, and psoas major become massive spinal compressors. Spinal compression, compression of joints in general, is dreadfully problematic, and is a common issue pelvic health patients deal with, whether they are consciously aware of it or not.
As far as the scalenes and QL’s go, both muscles attach at opposite ends of the rib cage and opposite ends of the sympathetic chain. The middle Scalene, the most accessible and easy scalene to target, attaches the first rib to the cervical spine, and the QL’s attach the twelfth rib to the pelvis. The scalenes are typically considered primary causers of thoracic outlet syndrome (TOS), which is true. However, what is not typically considered is how easy it is for the QL itself to cause TOS. Think about it. If the QL’s get tight, which they are in the majority of PT patients, especially pelvic health patients, they pull the entire rib cage down. This places tension on the scalenes and they get angry and tight. Now, we have the twelfth rib being pulled down and the first rib being pulled up. This happens in reverse order as well. Scalene pathology leading to lumbopelvic pathology. If either the scalenes or the QL’s are pathologic, the other often follows in short order, creating another negative feedback loop, further elevating sympathetic autonomic activity and disrupting normal pelvic function.
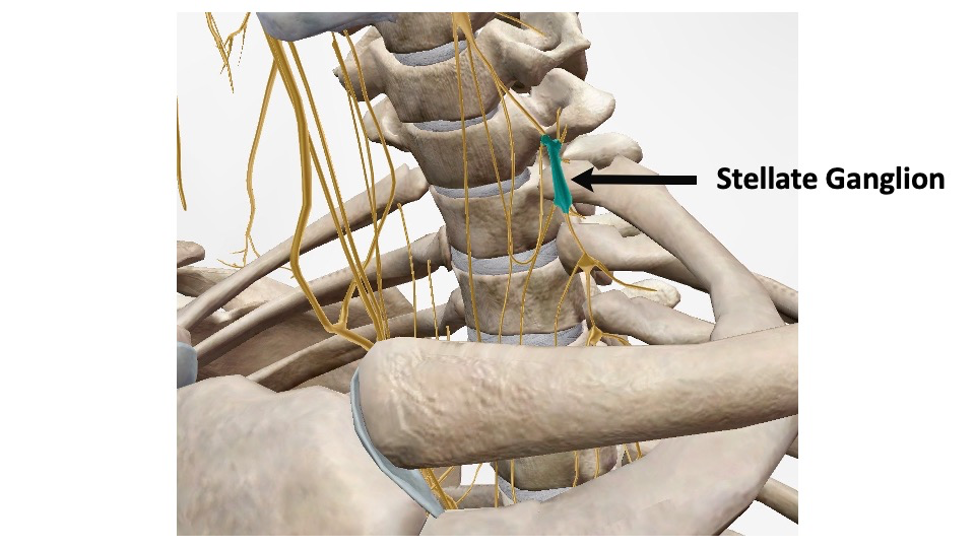
Another key thing to consider is the stellate ganglion, the superior ganglion of the sympathetic chain, sitting directly in front of the first rib attachment at C7-T1. Subsequently, first rib deviation, or tension on the chain coming from lower in the thoracolumbar spine, can cause serious aggravation of the stellate ganglion, short circuiting the entire SANS, making it hyperactive. This inhibits parasympathetic function, which inhibits the parasympathetically innervated pelvic floor muscles, leading to pain and dysfunction. This is a good example of why it is necessary to treat the body as a whole, cohesive unit, and why treating localized areas on their own is far less effective.
The multifidus crosses the entire sympathetic chain and the psoas major crosses most of it. These two muscles, when pathologic and short, most directly place stress on the spine, sympathetic chain and spinal nerve roots. The multifidus, in cases of chronic back pain, regardless of the cause, becomes infiltrated with adipose tissue. A freaking lot of it, causing widespread panic of the sympathetics. When the multifidus, our primary posterior spinal stabilizer, stops working, our bigger, fast twitch muscles like the latissimus and the trapezius try to do the multifidus’ job for it. Lazy, no good, tub-o-lard multifidus! The multifidus is made to constantly fire throughout the day to provide dynamic, functional spinal stability. Those other muscles are not. When different, faster twitch muscles try to do a job they are not meant for, they get tired and cranky real quick-like. This further deviates the spine, disrupting the sympathetic chain, leading to SANS hyperactivity and pelvic dysfunction. Needling combined with manipulation are the fastest way to reverse these processes.
The overall end result of chronic pathology in these structures, of mental and physical pathology in general, is SANS stimulation, PANS depression, and dysregulation of the ANS, possibly the single most detrimental, underlying factor responsible for overall health degradation. Departure from ANS homeostasis can cause just about any chronic impairment you can think of. Chronic idiopathic pain is a common one. Now, this seems simple, and it is. To solve a problem, like to actually fix it so it doesn’t come right back, the underlying cause, or causes, of said problem must be addressed. Duh, I know, right? Unfortunately, this hardly ever happens in typical medicine, especially for chronic conditions, like pain. A lot of chronic pain cases begin with a specific cause, but once the obvious causative factor is removed, the pain persists. This is because the body and mind were unable, for whatever reason, to restore homeostasis following the acute insult, leading to dysfunction.
Now, if the ANS has gone haywire and stuff hurts or doesnt work for any apparent reason, whatever caused the problem in the first place becomes irrelevant. The best way to address chronic idiopathic pain is to help the mind and body heal themselves. One of the simplest ways to do this, as mentioned above, is to remove as many sympathetic stressors from neuromusculoskeletal tissue as possible, while at the same time targeting the parasympathetics. Wherever the pathologic tissues and joints are located, treating the pelvic floor musculature is one of the best ways to stimulate the PANS and nudge the ANS toward homeostasis.
Everyone has some type of pathologic tissue in the pelvic floor structures. Removing tissue pathology alone, anywhere in the body, whether it’s causing conscious discomfort or not, removes sympathetic stress on the ANS. The unique thing about the pelvic floor muscles is they are innervated by the parasympathetic dominant portion of our ANS, S2-S4. This means that even without tissue pathology, treating the pelvic floor remains a powerful area to stimulate with electrical dry needling to specifically stimulate the PANS. This helps the brain help the body and vice versa. ANS homeostasis allows the mind and body the best chance to heal themselves. The therapeutic effect of this is immense and should not be discounted.
Everything in our body is intricately interconnected, and we don’t understand most of it. One thing we are pretty sure about, however, is the human body’s natural response to most impairments; sympathetic elevation with concomitant parasympathetic depression. We also know the overall effect of needling, almost regardless of how it is performed, is parasympathetic dominance compared to baseline. The sympathetic and parasympathetic portions of the ANS can and should be targeted throughout the body to achieve optimal results for any condition.
Almost nothing in the human body is effectively treated on its own, as a stand-alone treatment, including erectile dysfunction and other male pelvic health impairments. The body and mind must be addressed as a cohesive, functional system, rather than solely focusing on muscles directly in the area of complaint, for example, although that is certainly part of the battle. This is why so many medical treatments never actually fix anything, and rather, function as temporary maskers of impairment. Viagra is a good example of this, especially since a large percentage of erectile dysfunction occurs in the absence of specific tissue damage. Otherwise known as an idiopathic dysfunctional dingy… It only addresses a symptom of erectile dysfunction, decreased blood flow, by temporarily improving nitrous oxide availability, which increases blood flow and muscle function. Temporarily. Most medical interventions are too narrowly focused and don’t address any underlying causative factors. This is one reason we struggle to truly cure medical pathology.
Another unique thing about the pelvic floor muscles is they are almost impossible to stretch. The obturator internus is really the only one we can stretch because it attaches on the greater trochanter of the femur. The other muscles attach in between different parts of the pelvis, which does not move much. The most effective way to lengthen any muscle is to needle it, followed by joint manipulation and stretching. Most of the time, stretching is not needed after needling and manipulation. They are our two most powerful tools in removing trigger points and normalizing tissue length, which you must achieve to treat pelvic pain and induce ANS homeostasis. The pelvic floor musculature often only responds in a meaningful way to direct treatment, and the only direct treatment we can perform on any muscle is with needles. Anything else is indirect and less effective, as you have to treat through the skin and other superficial musculature. Remember, the joints surrounding the pelvic floor and throughout the spine need to be reduced to neutral following needling to maximize treatment efficacy and homeostasis.
Overall, we understand a small percentage of the specific mechanisms of action in between the cause and effect of medical treatments. What we do understand, we think, are a few of the basic driving factors behind mental and physical impairment. Sympathetic autonomic hyperactivity being the most common thread. Unfortunately, these common threads are often disregarded in the actual treatment of pathology. Fortunately, one of the most objective facts we have gleaned about dry needling and joint manipulation, especially when combined and thoughtfully performed, is their homeostatic effect on the ANS via sympathetic depression and parasympathetic elevation. I believe the combination of these tools is one of the most powerful medical treatments to improve ANS homeostasis. What I know for a fact is this: you will never achieve your full recovery potential from any medical impairment, including pelvic health impairments, without targeted regulation of the ANS toward homeostasis, the key to health.
If you are a guy struggling with pelvic health impairment, there is hope. Once thoughtful needling combined with joint manipulation are implemented, a large percentage of men go from pelvically impaired to fully functional. I witness this on a weekly basis with my patients and medical practitioner students. This is an awesome, life-changing event that will reciprocally improve many other impairments, including mental health impairments.
Let me know if anyone has any questions about anything. If you are a practitioner looking to advance your treatment strategies, or a person looking for help with a specific issue, we are happy to help. Thanks.
Jason
DISCLAIMER: The content on the blog for Intricate Art Spine & Body Solutions, LLC is for educational and informational purposes only, and is not intended as medical advice. The information contained in this blog should not be used to diagnose, treat or prevent any disease or health illness. Any reliance you place on such information is therefore strictly at your own risk. Please consult with your physician or other qualified healthcare professional before acting on any information presented here.
References
Pelvic Floor
-
Ferri-Morales, A., 2018. Posterior tibial nerve stimulation in the treatment of fecal incontinence: a systematic review. Rev Esp Enferm Dig, 110(9), pp.577-588. -
Liu, B., Liu, Y., Qin, Z., Zhou, K., Xu, H., He, L., Li, N., Su, T., Sun, J., Yue, Z. and Zang, Z., 2019, January. Electroacupuncture versus pelvic floor muscle training plus solifenacin for women with mixed urinary incontinence: a randomized noninferiority trial. In Mayo Clinic Proceedings (Vol. 94, No. 1, pp. 54-65). Elsevier. -
Wang, Y., Zhishun, L., Peng, W., Zhao, J. and Liu, B., 2013. Acupuncture for stress urinary incontinence in adults. Cochrane Database of Systematic Reviews, (7). -
Itza, F., Zarza, D., Serra, L., Gomez-Sancha, F., Salinas, J. and Allona-Almagro, A., 2010. Myofascial pain syndrome in the pelvic floor: a common urological condition. Actas Urológicas Españolas (English Edition), 34(4), pp.318-326. -
Kalichman, L. and Vulfsons, S., 2010. Dry needling in the management of musculoskeletal pain. The Journal of the American Board of Family Medicine, 23(5), pp.640-646. -
Dunning, J., Butts, R., Mourad, F., Young, I., Flannagan, S. and Perreault, T., 2014. Dry needling: a literature review with implications for clinical practice guidelines. Physical therapy reviews, 19(4), pp.252-265. -
Montenegro, M.L., Braz, C.A., Rosa-e-Silva, J.C., Candido-dos-Reis, F.J., Nogueira, A.A. and Poli-Neto, O.B., 2015. Anaesthetic injection versus ischemic compression for the pain relief of abdominal wall trigger points in women with chronic pelvic pain. BMC anesthesiology, 15(1), p.175. -
Halle, J.S. and Halle, R.J., 2016. Pertinent dry needling considerations for minimizing adverse effects–part two. International journal of sports physical therapy, 11(5), p.810. -
Zhong, D., Tang, W., Geng, D. and He, C., 2019. Efficacy and safety of acupuncture therapy for urinary incontinence in women: A systematic review and meta-analysis. Medicine, 98(40). -
Zhang, Z., Wang, W., Song, Y., Zhai, T., Zhu, Y., Jiang, L., Li, Q., Jin, L., Li, K. and Feng, W., 2021. Immediate Effect of Dry Needling at Myofascial Trigger Point on Hand Spasticity in Chronic Post-stroke Patients: A Multicenter Randomized Controlled Trial. Frontiers in neurology, 12. -
Sheikhhoseini, R. and Arab, A.M., 2018. Dry needling in myofascial tracks in non-relaxing pelvic floor dysfunction: A case study. Journal of Bodywork and Movement Therapies, 22(2), pp.337-340. -
George, A., VanEtten, L. and Briggs, M., 2018. Dry Needling for Female Chronic Pelvic Pain: A Case Series. Journal of Women's Health Physical Therapy, 42(1), pp.8-16. -
Lin, A., Abbas, H., Sultan, M. and Tzeng, T., 2022. A critical review of interventional treatments for myofascial pelvic pain. -
Bubnov, R. and Kalika, L., Dry needling of trigger points under ultrasound guidance effective to treat chronic pelvic pain and pelvic prolapse. -
Frederice, C.P., Brito, L.G.O., Pereira, G.M.V., Lunardi, A.L.B. and Juliato, C.R.T., 2021. Interventional treatment for myofascial pelvic floor pain in women: systematic review with meta-analysis. International Urogynecology Journal, 32(5), pp.1087-1096. -
Rajkannan, P. and Vijayaraghavan, R., 2019. Dry needling in chronic abdominal wall pain of uncertain origin. Journal of Bodywork and Movement Therapies, 23(1), pp.94-98. -
Alappattu, M., Hilton, S. and Bishop, M., 2019. An international survey of commonly used interventions for management of pelvic pain. Journal of women's health physical therapy, 43(2), p.82. -
Bartley, J., Han, E., Gupta, P., Gaines, N., Killinger, K.A., Boura, J.A., Farrah, M., Gilleran, J., Sirls, L.T. and Peters, K.M., 2019. Transvaginal trigger point injections improve pain scores in women with pelvic floor hypertonicity and pelvic pain conditions. Female pelvic medicine & reconstructive surgery, 25(5), pp.392-396. -
Hastings, J. and Machek, M., 2020. Pelvic Floor Dysfunction in Women. Current Physical Medicine and Rehabilitation Reports, 8(2), pp.64-75. -
Bazzaz-Yamchi, M., Naghdi, S., Nakhostin-Ansari, A., Hadizadeh, M., Ansari, N.N., Moghimi, E. and Hasson, S., 2021. Acute and Short-Term Effects of Dry Needling in Patients with Chronic Nonspecific Low Back Pain and Hamstring Tightness: A Pilot Study. The Scientific World Journal, 2021.
Men’s Health
-
Ferrini, M.G., Gonzalez-Cadavid, N.F. and Rajfer, J., 2017. Aging related erectile dysfunction—potential mechanism to halt or delay its onset. Translational andrology and urology, 6(1), p.20. -
Wang, J.S., Deng, S., Zhao, Q., Zhang, K.G., Bao, B.H., Feng, J.L., Meng, F.C., Dai, H.H., Li, X., Li, H.S. and Wang, B., 2021. A Bioinformatic Investigation of the Mechanism Underlying Migraine-Induced Erectile Dysfunction. BioMed Research International, 2021. -
Wang, H., Zhao, M., Zhang, J., Yan, B., Liu, S., Zhao, F., Guo, J. and Wang, F., 2022. The Efficacy of Acupuncture on Patients with Erectile Dysfunction: A Review. Evidence-Based Complementary and Alternative Medicine, 2022. -
Wang, J., Zhou, Y., Dai, H., Bao, B., Dang, J., Li, X., Wang, B. and Li, H., 2019. The safety and efficacy of acupuncture for erectile dysfunction: A network meta-analysis. Medicine, 98(2). -
Evren, I., ÖZTEKİN, İ., Atayoglu, A.T. and BUCCHOLZ, N., 2021. Comparison of Medical Treatment and Acupuncture in Treatment of Psychogenic Erectile Dysfunction: a Prospective, Randomized, Placebo-Controlled Study. International Journal of Traditional and Complementary Medicine Research, 2(3), pp.121-125. -
Lai, B.Y., Cao, H.J., Yang, G.Y., Jia, L.Y., Grant, S., Fei, Y.T., Wong, E., Li, X.L., Yang, X.Y. and Liu, J.P., 2019. Acupuncture for treatment of erectile dysfunction: a systematic review and meta-analysis. The World Journal of Men's Health, 37(3), p.322.
Vagus Nerve Stimulation
-
Butt, M.F., Albusoda, A., Farmer, A.D. and Aziz, Q., 2020. The anatomical basis for transcutaneous auricular vagus nerve stimulation. Journal of anatomy, 236(4), pp.588-611. -
Garner, B.K., Hopkinson, S.G., Ketz, A.K., Landis, C.A. and Trego, L.L., 2018. Auricular acupuncture for chronic pain and insomnia: a randomized clinical trial. Medical acupuncture, 30(5), pp.262-272. -
Jaić, K.K., Turković, T.M., Pešić, M., Djaković, I., Košec, V. and Košec, A., 2019. Auricular acupuncture as effective pain relief after episiotomy: a randomized controlled pilot study. Archives of gynecology and obstetrics, 300(5), pp.1295-1301 -
Johnson, R.L. and Wilson, C.G., 2018. A review of vagus nerve stimulation as a therapeutic intervention. Journal of inflammation research, 11, p.203. -
Kang, H.R., Lee, Y.S., Kim, H.R., Kim, E.J., Kim, K.H., Kim, K.S., Jung, C.Y. and Lee, J.K., 2017. A clinical study of electroacupuncture and auricular acupuncture for abdominal pain relief in patients with pancreatitis: A pilot study. Korean Journal of Acupuncture, 34(1), pp.47-55. -
Moura, C.D.C., Chaves, E.D.C.L., Cardoso, A.C.L.R., Nogueira, D.A., Azevedo, C. and Chianca, T.C.M., 2019. Auricular acupuncture for chronic back pain in adults: a systematic review and metanalysis. Revista da Escola de Enfermagem da USP, 53. -
Sator-Katzenschlager, S.M., Szeles, J.C., Scharbert, G., Michalek-Sauberer, A., Kober, A., Heinze, G. and Kozek-Langenecker, S.A., 2003. Electrical stimulation of auricular acupuncture points is more effective than conventional manual auricular acupuncture in chronic cervical pain: a pilot study. Anesthesia & Analgesia, 97(5), pp.1469-1473. -
Shah, A.N., Moore, C.B. and Brigger, M.T., 2020. Auricular acupuncture for adult tonsillectomy. The Laryngoscope, 130(8), pp.1907-1912. -
Sprouse-Blum, A.S., Smith, G., Sugai, D. and Parsa, F.D., 2010. Understanding endorphins and their importance in pain management. Hawaii medical journal, 69(3), p.70. -
Taylor, S.L., Giannitrapani, K.F., Ackland, P.E., Thomas, E.R., Federman, D.G., Holliday, J.R., Olson, J., Kligler, B. and Zeliadt, S.B., 2021. The Implementation and Effectiveness of Battlefield Auricular Acupuncture for Pain. Pain Medicine. -
Tsai, S.L., Fox, L.M., Murakami, M. and Tsung, J.W., 2016. Auricular acupuncture in emergency department treatment of acute pain. Annals of emergency medicine, 68(5), pp.583-585. -
Usichenko, T.I., Dinse, M., Hermsen, M., Witstruck, T., Pavlovic, D. and Lehmann, C., 2005. Auricular acupuncture for pain relief after total hip arthroplasty–a randomized controlled study. Pain, 114(3), pp.320-327. -
Usichenko, T.I., Kuchling, S., Witstruck, T., Pavlovic, D., Zach, M., Hofer, A., Merk, H., Lehmann, C. and Wendt, M., 2007. Auricular acupuncture for pain relief after ambulatory knee surgery: a randomized trial. Cmaj, 176(2), pp.179-183. -
Usichenko, T.I., Lehmann, C. and Ernst, E., 2008. Auricular acupuncture for postoperative pain control: a systematic review of randomised clinical trials. Anaesthesia, 63(12), pp.1343-1348. -
Yeh, C.H., Chiang, Y.C., Hoffman, S.L., Liang, Z., Klem, M.L., Tam, W.W., Chien, L.C. and Suen, L.K.P., 2014. Efficacy of auricular therapy for pain management: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine, 2014. -
Prescott, S.L. and Liberles, S.D., 2022. Internal senses of the vagus nerve. Neuron. -
Badran, B.W., Brown, J.C., Dowdle, L.T., Mithoefer, O.J., LaBate, N.T., Coatsworth, J., DeVries, W.H., Austelle, C.W., McTeague, L.M., Yu, A. and Bikson, M., 2018. Tragus or cymba conchae? Investigating the anatomical foundation of transcutaneous auricular vagus nerve stimulation (taVNS). Brain stimulation, 11(4), p.947. -
Bonaz, B., Sinniger, V. and Pellissier, S., 2021. Therapeutic potential of vagus nerve stimulation for inflammatory bowel diseases. Frontiers in neuroscience, 15, p.300. -
Burger, A.M., D’Agostini, M., Verkuil, B. and Van Diest, I., 2020. Moving beyond belief: A narrative review of potential biomarkers for transcutaneous vagus nerve stimulation. Psychophysiology, 57(6), p.e13571. -
Ottaviani, M.M., Wright, L., Dawood, T. and Macefield, V.G., 2020. In vivo recordings from the human vagus nerve using ultrasound‐guided microneurography. The Journal of physiology, 598(17), pp.3569-3576.
Autonomic Nervous System
-
Uchida C, Waki H, Minakawa Y, Tamai H, Hisajima T, Imai K. Evaluation of Autonomic Nervous System Function Using Heart Rate Variability Analysis During Transient Heart Rate Reduction Caused by Acupuncture. Med Acupunct. 2018 Apr 1;30(2):89-95. doi: 10.1089/acu.2017.1266. PMID: 29682149; PMCID: PMC5908425. -
Jin, B.X., Jin, L.L. and Jin, G.Y., 2019. The anti-inflammatory effect of acupuncture and its significance in analgesia. World Journal of Acupuncture-Moxibustion, 29(1), pp.1-6. -
An, S. and Keum, D., 2021. Effect of Acupuncture at the Field of the Auricular Branch of the Vagus Nerve on Autonomic Nervous System Change. Journal of Korean Medicine Rehabilitation, 31(2), pp.81-97. -
Zhou C, Bao J, Hu H, Ye S, Shao X, Liang Y, Fang J. Acupuncture Based on Regulating Autonomic Nerves for the Prevention of Migraine Without Aura: A Prospective, Double-Dummy, Randomized Controlled Clinical Trial. J Pain Res. 2022 Aug 4;15:2211-2221. doi: 10.2147/JPR.S372311. PMID: 35957963; PMCID: PMC9359787. -
Uchida C, Waki H, Minakawa Y, Tamai H, Miyazaki S, Hisajima T, Imai K. Effects of Acupuncture Sensations on Transient Heart Rate Reduction and Autonomic Nervous System Function During Acupuncture Stimulation. Med Acupunct. 2019 Jun 1;31(3):176-184. doi: 10.1089/acu.2019.1350. Epub 2019 Jun 17. PMID: 31297171; PMCID: PMC6604907. -
Huang TI, Hsieh CL. Effects of Acupuncture on Oxidative Stress Amelioration via Nrf2/ARE-Related Pathways in Alzheimer and Parkinson Diseases. Evid Based Complement Alternat Med. 2021 Apr 26;2021:6624976. doi: 10.1155/2021/6624976. PMID: 33995547; PMCID: PMC8096560. -
Saha S, Buttari B, Panieri E, Profumo E, Saso L. An Overview of Nrf2 Signaling Pathway and Its Role in Inflammation. Molecules. 2020 Nov 23;25(22):5474. doi: 10.3390/molecules25225474. PMID: 33238435; PMCID: PMC7700122. -
Gevirtz, R. The Role of the Autonomic Nervous System in Headache: Biomarkers and Treatment. Curr Pain Headache Rep 26, 767–774 (2022). https://doi.org/10.1007/s11916-022-01079-x -
Li, Q.Q., Shi, G.X., Xu, Q., Wang, J., Liu, C.Z. and Wang, L.P., 2013. Acupuncture effect and central autonomic regulation. Evidence-Based Complementary and Alternative Medicine, 2013. -
Park, S.U., Jung, W.S., Moon, S.K., Park, J.M., Ko, C.N., Cho, K.H., Kim, Y.S. and Bae, H.S., 2008. Effects of acupuncture on autonomic nervous system in normal subjects under mental stress. The Journal of Korean Medicine, 29(2), pp.107-115. -
Haker, E., Egekvist, H. and Bjerring, P., 2000. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. Journal of the autonomic nervous system, 79(1), pp.52-59. -
Bäcker, M., Grossman, P., Schneider, J., Michalsen, A., Knoblauch, N., Tan, L., Niggemeyer, C., Linde, K., Melchart, D. and Dobos, G.J., 2008. Acupuncture in migraine: investigation of autonomic effects. The Clinical journal of pain, 24(2), pp.106-115. -
Uchida, C., Waki, H., Minakawa, Y., Tamai, H., Miyazaki, S., Hisajima, T. and Imai, K., 2019. Effects of acupuncture sensations on transient heart rate reduction and autonomic nervous system function during acupuncture stimulation. Medical acupuncture, 31(3), pp.176-184. -
Uchida, C., Waki, H., Minakawa, Y., Tamai, H., Miyazaki, S., Hisajima, T. and Imai, K., 2019. Effects of acupuncture sensations on transient heart rate reduction and autonomic nervous system function during acupuncture stimulation. Medical acupuncture, 31(3), pp.176-184. -
Butts, r., dunning, j. And serafino, c., 2020. Dry needling strategies for musculoskeletal conditions: do the number of needles and needle retention time matter? A narrative review of the literature. Journal of bodywork and movement therapies. -
Castro-Sánchez, A.M., Garcia-López, H., Fernández-Sánchez, M., Perez-Marmol, J.M., Leonard, G., Gaudreault, N., Aguilar-Ferrándiz, M.E. and Matarán-Peñarrocha, G.A., 2020. Benefits of dry needling of myofascial trigger points on autonomic function and photoelectric plethysmography in patients with fibromyalgia syndrome. Acupuncture in Medicine, 38(3), pp.140-149. -
Loaiza, L. A., Yamaguchi, S., Ito, M., & Ohshima, N. (2002). Electro-acupuncture stimulation to muscle afferents in anesthetized rats modulates the blood flow to the knee joint through autonomic reflexes and nitric oxide. Autonomic Neuroscience : Basic & Clinical, 97(2), 103–109. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12132642. -
Morikawa, Y., Takamoto, K., Nishimaru, H., Taguchi, T., Urakawa, S., Sakai, S., … Nishijo, H. (2017). Compression at myofascial trigger point on chronic neck pain provides pain relief through the prefrontal cortex and autonomic nervous system: A pilot study. Frontiers in Neuroscience, 11(APR). https://doi.org/10.3389/fnins.2017.00186. -
Sillevis, R., Van Duijn, J., Shamus, E. and Hard, M., 2021. Time effect for in-situ dry needling on the autonomic nervous system, a pilot study. Physiotherapy theory and practice, 37(7), pp.826-834. -
Lázaro-Navas, I., Lorenzo-Sánchez-Aguilera, C., Pecos-Martín, D., Jiménez-Rejano, J.J., Navarro-Santana, M.J., Fernández-Carnero, J. and Gallego-Izquierdo, T., 2021. Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(11), p.6018. -
Abbaszadeh-Amirdehi, M., Ansari, N.N., Naghdi, S., Olyaei, G. and Nourbakhsh, M.R., 2017. Therapeutic effects of dry needling in patients with upper trapezius myofascial trigger points. Acupuncture in Medicine, 35(2), pp.85-92. -
Castro-Sánchez, A.M., Garcia-López, H., Fernández-Sánchez, M., Perez-Marmol, J.M., Leonard, G., Gaudreault, N., Aguilar-Ferrándiz, M.E. and Matarán-Peñarrocha, G.A., 2020. Benefits of dry needling of myofascial trigger points on autonomic function and photoelectric plethysmography in patients with fibromyalgia syndrome. Acupuncture in Medicine, 38(3), pp.140-149. -
Skorupska, E., Rychlik, M. and Samborski, W., 2015. Intensive vasodilatation in the sciatic pain area after dry needling. BMC complementary and alternative medicine, 15(1), pp.1-9. -
Clark, N.G., Hill, C.J., Koppenhaver, S.L., Massie, T. and Cleland, J.A., 2021. The effects of dry needling to the thoracolumbar junction multifidi on measures of regional and remote flexibility and pain sensitivity: A randomized controlled trial. Musculoskeletal Science and Practice, 53, p.102366. -
Sánchez-Infante, J., Navarro-Santana, M.J., Bravo-Sánchez, A., Jiménez-Diaz, F. and Abián-Vicén, J., 2021. Is Dry Needling Applied by Physical Therapists Effective for Pain in Musculoskeletal Conditions? A Systematic Review and Meta-Analysis. Physical Therapy, 101(3), p.pzab070. -
Eftekharsadat, B., Babaei-Ghazani, A. and Zeinolabedinzadeh, V., 2016. Dry needling in patients with chronic heel pain due to plantar fasciitis: A single-blinded randomized clinical trial. Medical journal of the Islamic Republic of Iran, 30, p.401. -
Li, Q.Q., Shi, G.X., Xu, Q., Wang, J., Liu, C.Z. and Wang, L.P., 2013. Acupuncture effect and central autonomic regulation. Evidence-Based Complementary and Alternative Medicine, 2013. -
Mori, H., Nishijo, K., Kawamura, H. and Abo, T., 2002. Unique immunomodulation by electro-acupuncture in humans possibly via stimulation of the autonomic nervous system. Neuroscience Letters, 320(1-2), pp.21-24. -
Sakatani, K., Kitagawa, T., Aoyama, N. and Sasaki, M., 2010. Effects of acupuncture on autonomic nervous function and prefrontal cortex activity. In Oxygen Transport to Tissue XXXI (pp. 455-460). Springer, Boston, MA -
Haker, E., Egekvist, H. and Bjerring, P., 2000. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. Journal of the autonomic nervous system, 79(1), pp.52-59. -
Shu, Q., Wang, H., Litscher, D., Wu, S., Chen, L., Gaischek, I., Wang, L., He, W., Zhou, H., Litscher, G. and Liang, F., 2016. Acupuncture and moxibustion have different effects on fatigue by regulating the autonomic nervous system: a pilot controlled clinical trial. Scientific reports, 6(1), pp.1-11. -
Matić, Z. and Bojić, T., 2020. Acupuncture, autonomic nervous system and biophysical origin of acupuncture system. Vojnosanitetski pregled, 77(1), pp.79-86. -
Uchida, C., Waki, H., Minakawa, Y., Tamai, H., Hisajima, T. and Imai, K., 2018. Evaluation of autonomic nervous system function using heart rate variability analysis during transient heart rate reduction caused by acupuncture. Medical acupuncture, 30(2), pp.89-95. -
Napadow, V., Beissner, F., Lin, Y., Chae, Y. and Harris, R.E., 2020. Neural Substrates of Acupuncture: From Peripheral to Central Nervous System Mechanisms. Frontiers in neuroscience, 13, p.1419. -
An, S. and Keum, D., 2021. Effect of Acupuncture at the Field of the Auricular Branch of the Vagus Nerve on Autonomic Nervous System Change. Journal of Korean Medicine Rehabilitation, 31(2), pp.81-97. -
Kupari, J. and Ernfors, P., 2020. Pricking into Autonomic Reflex Pathways by Electrical Acupuncture. Neuron, 108(3), pp.395-397. -
Kurita, K., Kiyomitsu, K., Ogasawara, C., Mishima, R., Ogawa-Ochiai, K. and Tsumura, N., 2019. Effect of acupuncture on the autonomic nervous system as evaluated by non-contact heart rate variability measurement. Artificial Life and Robotics, 24(1), pp.19-23. -
Dommerholt, J., Hooks, T., Chou, L.W. and Finnegan, M., 2019. A critical overview of the current myofascial pain literature–November 2018. Journal of bodywork and movement therapies, 23(1), pp.65-73. -
Morikawa, Y., Takamoto, K., Nishimaru, H., Taguchi, T., Urakawa, S., Sakai, S., Ono, T. and Nishijo, H., 2017. Compression at myofascial trigger point on chronic neck pain provides pain relief through the prefrontal cortex and autonomic nervous system: a pilot study. Frontiers in neuroscience, 11, p.186. -
Dommerholt, J., Mayoral, O. and Thorp, J.N., 2021. A critical overview of the current myofascial pain literature–January 2021.
DISCLAIMER: The content on the blog for Intricate Art Spine & Body Solutions, LLC is for educational and informational purposes only, and is not intended as medical advice. The information contained in this blog should not be used to diagnose, treat or prevent any disease or health illness. Any reliance you place on such information is therefore strictly at your own risk. Please consult with your physician or other qualified healthcare professional before acting on any information presented here.
Stay Engaged With Intricate Art
Get the latest news, updates and offers from Intricate Art delivered to your inbox.